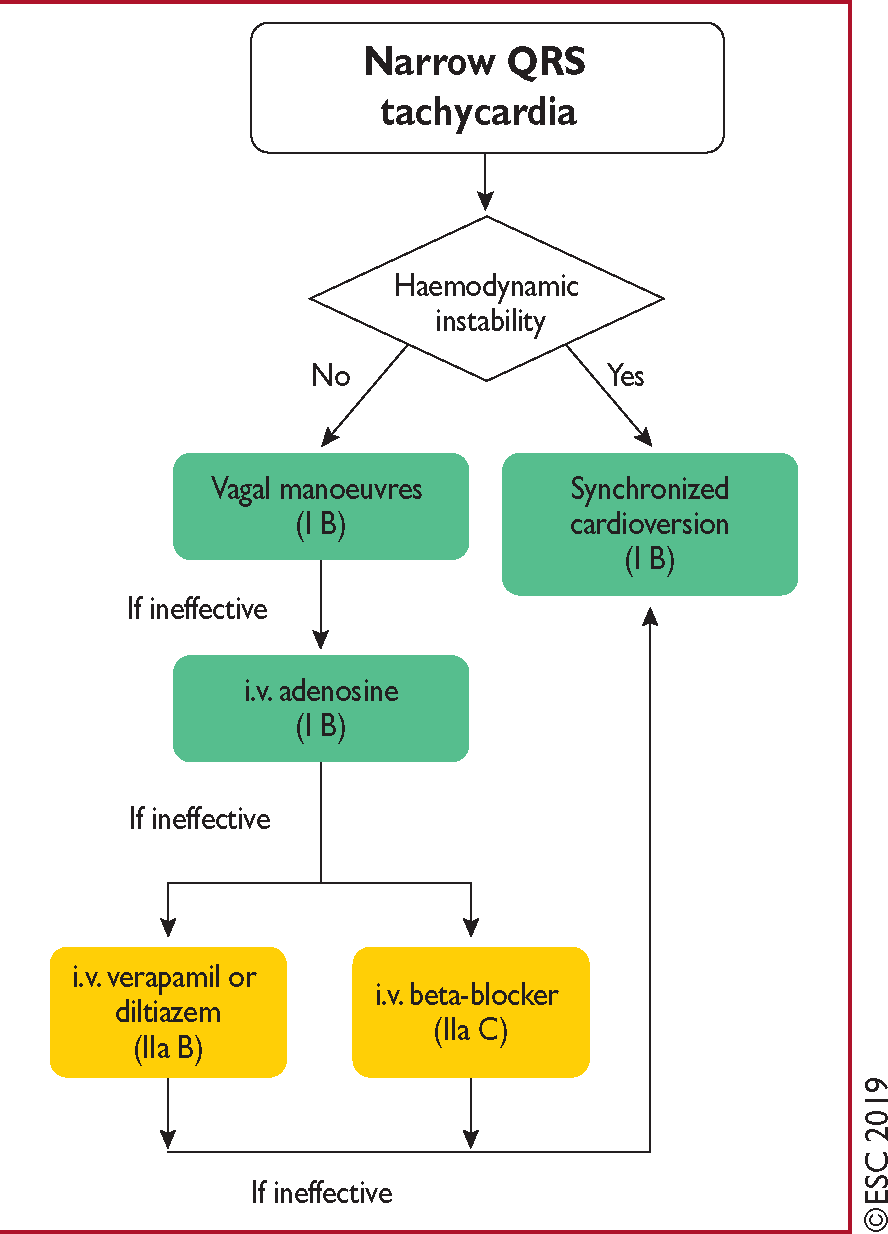
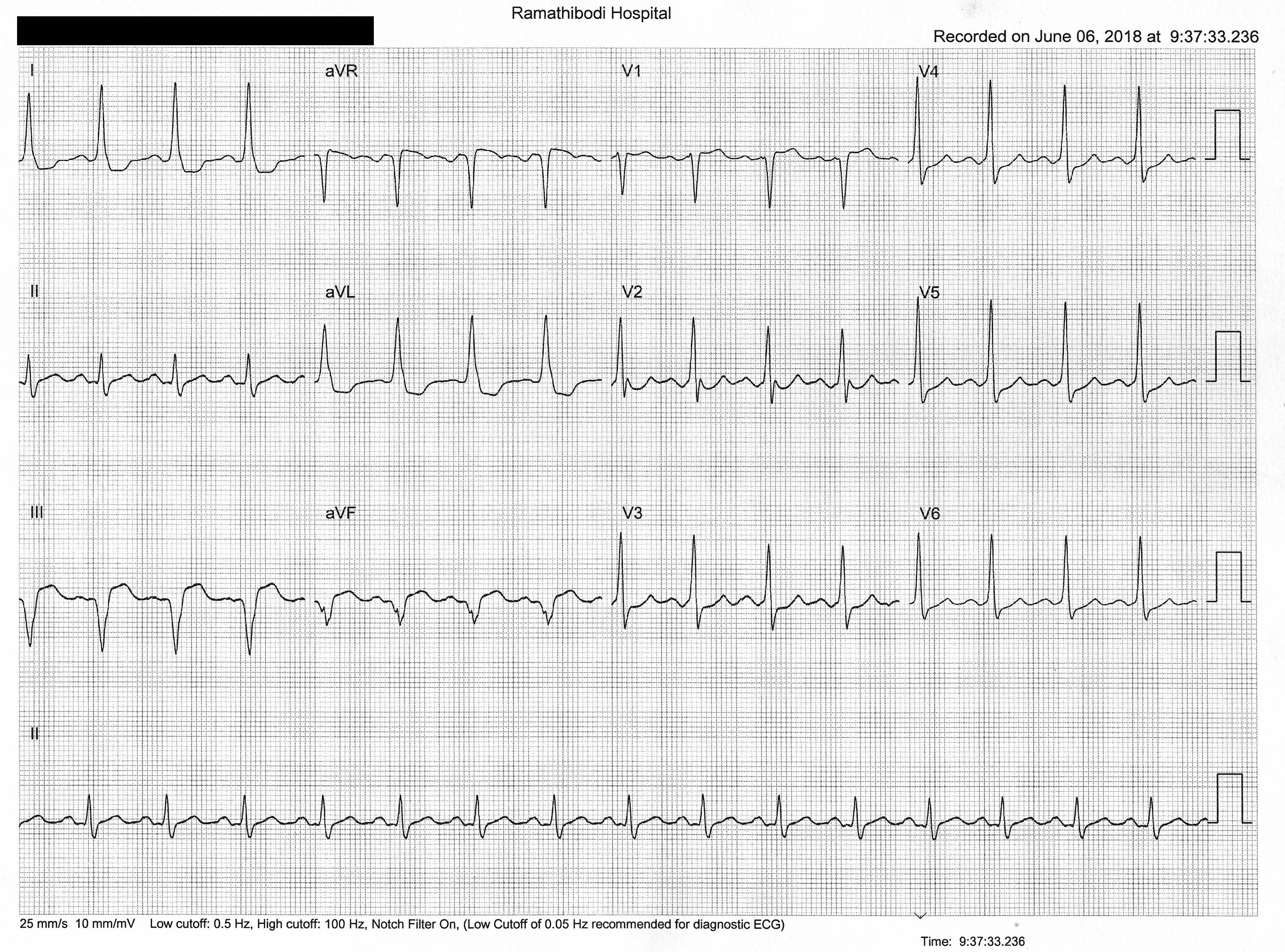
Acute Management of Narrow Complex Tachycardia
• Vagal manuever, Adenosine, CV
• BB, CCB
• NO AMIODARONE OR DIGOXIN
• BB, CCB
• NO AMIODARONE OR DIGOXIN
 For prevention of SVT in pregnant women,
For prevention of SVT in pregnant women,