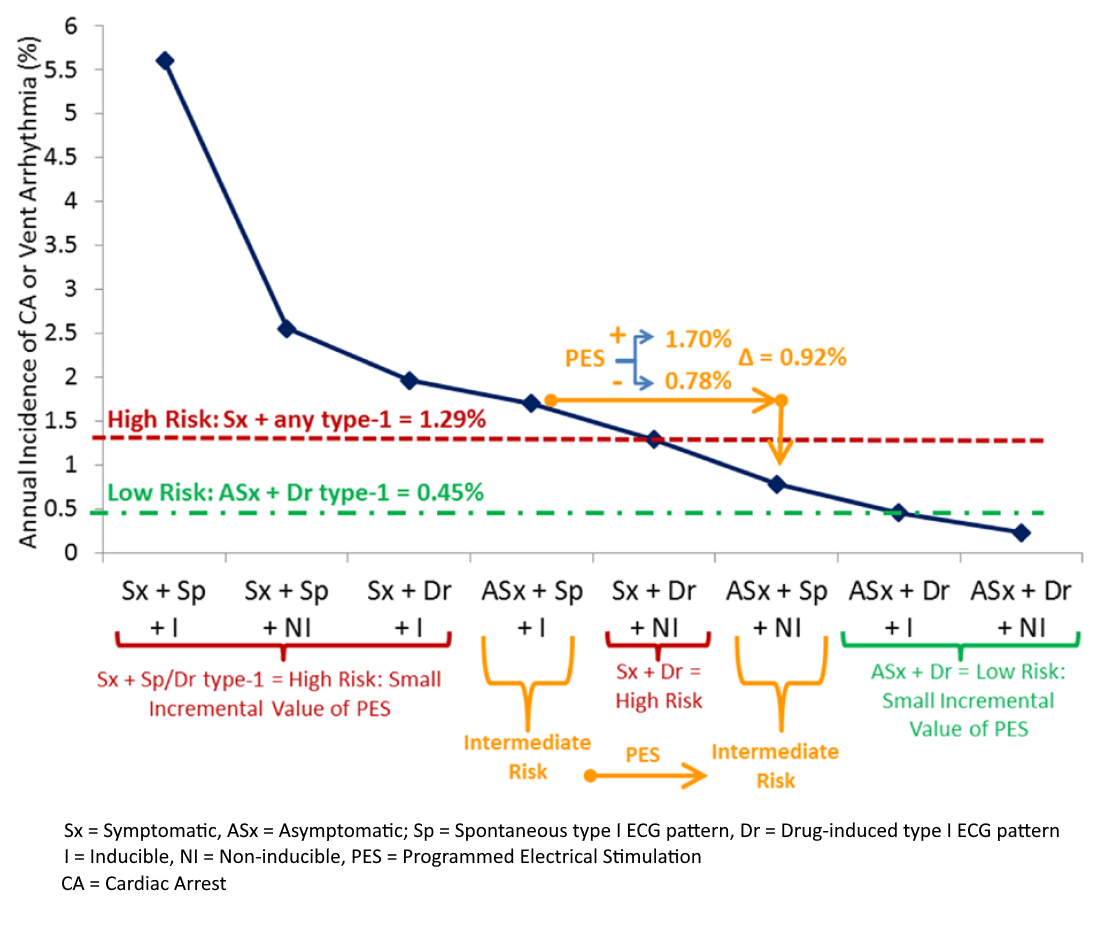
In individuals with high or low risk clinical features, EP study provided limited incremental prognostic value.
In intermediate risk group, inducible EP study would increase risk of malignant arrhythmia to 1.7%/year
and an ICD would be recommended.
If, however, the patient is non-inducible, the risk would be lower, 0.78%, but not sufficiently low
enough.