 heartRhythmBox
heartRhythmBox
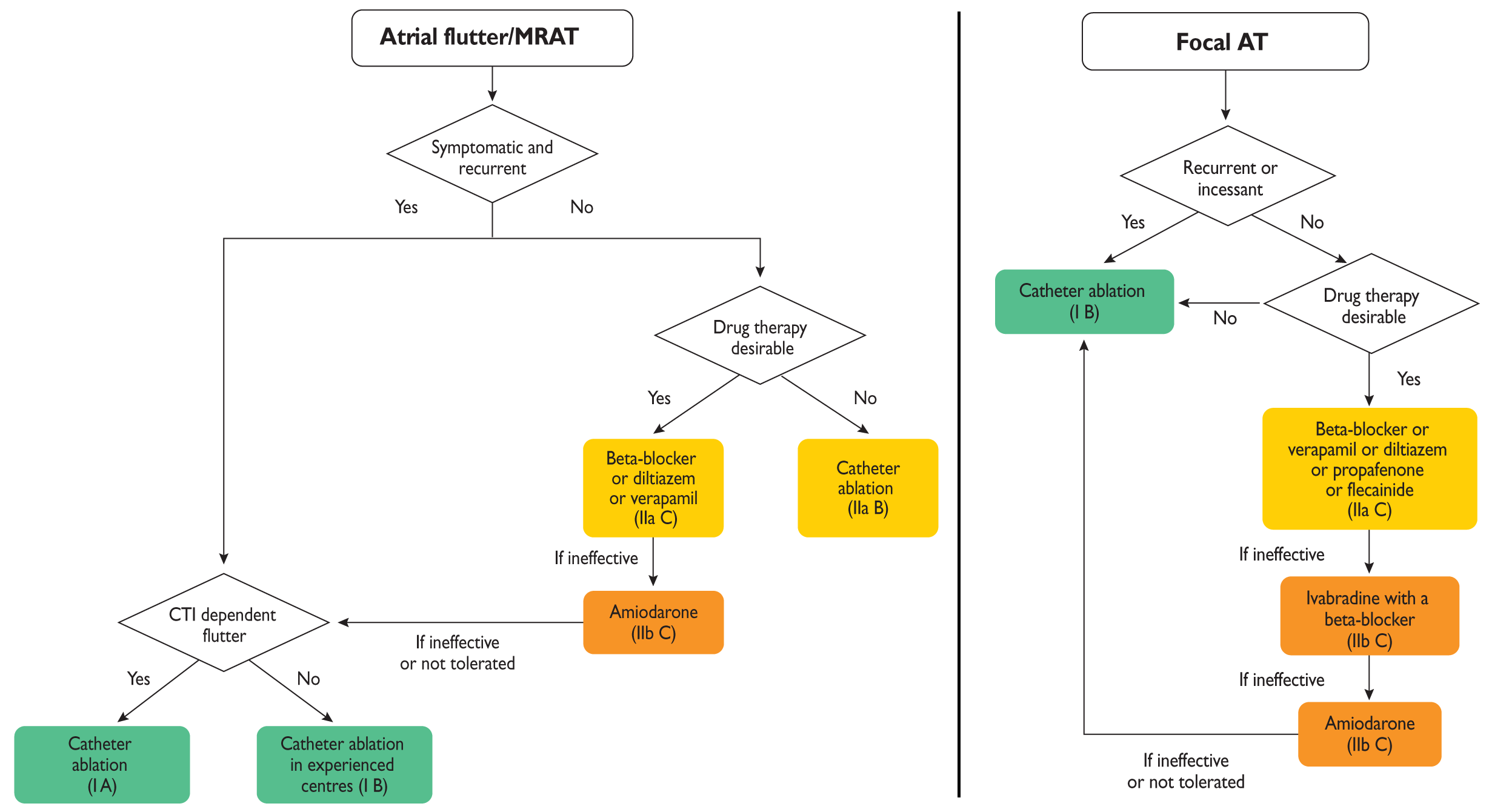
ทั้ง 3 ภาวะนี้ต่างกันที่กลไกการเกิด
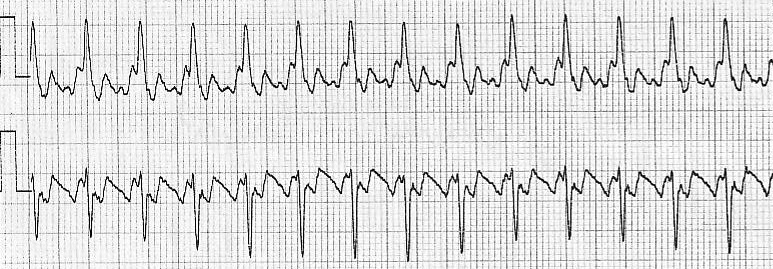
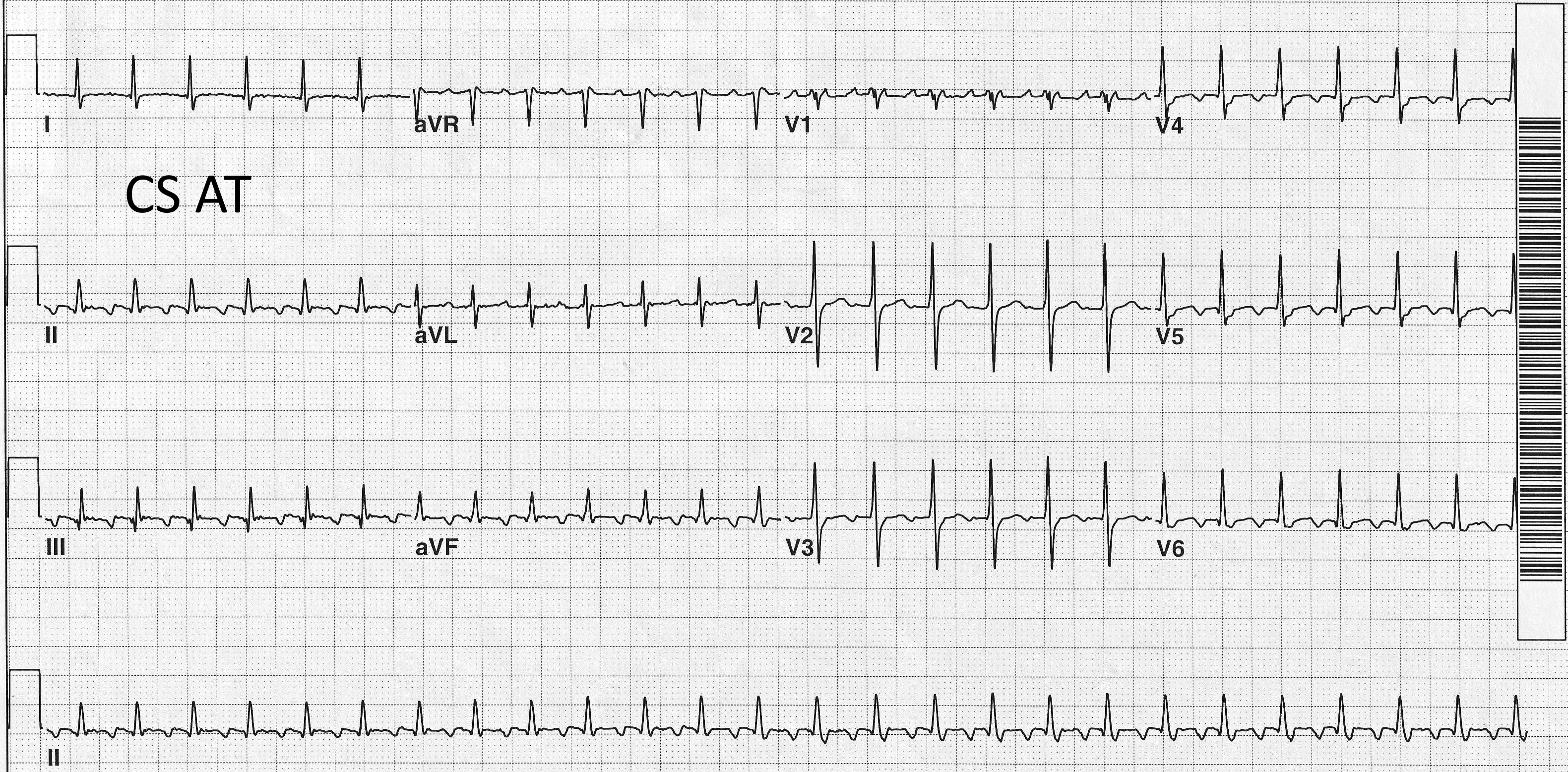
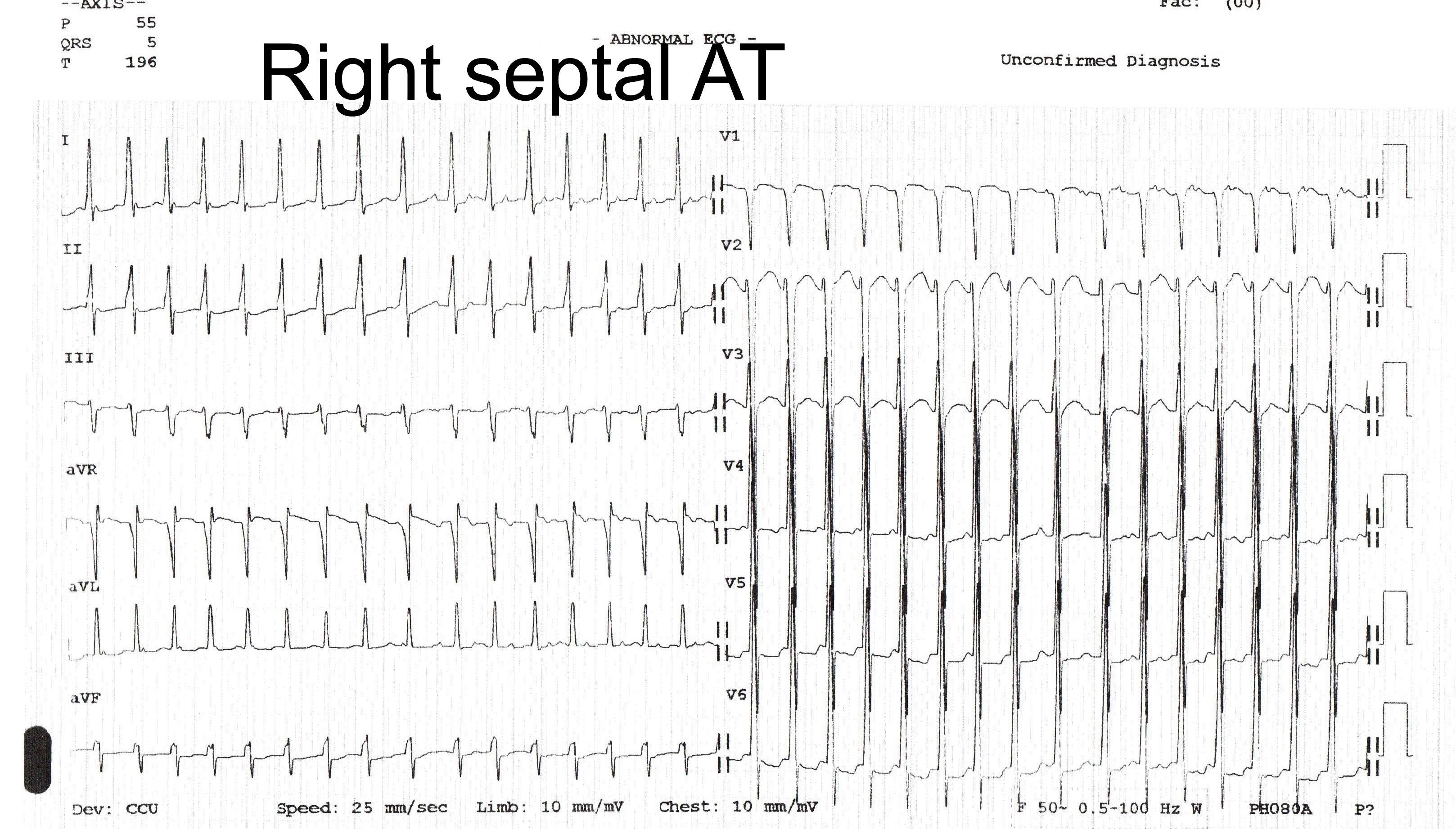
ถ้าดูจาก EKG ในคนที่เป็น AFL หรือ AT จะเห็น P wave ที่มีรูปร่างชัดเจนและสม่ำเสมอกว่าคนที่เป็น AF
ทั้ง 3 ภาวะนี้ อาจมี ventricular rate ที่สม่ำเสมอหรือไม่สม่ำเสมอก็ได้
A
| Characters | Focal | Microreentry | Macroreentry |
|---|---|---|---|
| Most Common heart diseases | None | AF s/p RFA | CAD, AF s/p RFA |
| ECG isoelectric interval | Yes | Yes | No |
| Record from >80% of CL | No | Yes | Yes |
| Entrain with PPI-TCL<20ms, 2sites >2cm apart | No | No | Yes |
| Activation Pattern | Radial | Radial | Large Loop |
| Ablation Approach | Focal | Focal | Linear |